A woman with fibroids is no more at risk for any kind of cancer than any other woman.
– Dr. Stanley West
Don’t let yourself be frightened into an unnecessary hysterectomy. If you have fibroids and need surgery, the appropriate operation is myomectomy, not hysterectomy.
– Dr. Stanley West
You have fibroid tumors, which I can assure you, are benign.
– Dr. Stanley West
Learn More
Dr. Stanley West is the author of The Hysterectomy Hoax, published in January, 1994 by Doubleday. In it he explains why 90 percent of all hysterectomies are unnecessary, and describes all the treatment options available to every woman, no matter what age.
Questions?
Contact Dr. West. He will answer you promptly


If your life is being negatively impacted by the presence of uterine fibroids, Dr. West is your best resource.
–Linda Congdon, RN, Preston, CT
For once after a doctor's visit, I left filled with enthusiasm, not paralyzing depression and fear...I could not have asked for a better outcome…[Dr. West is] the epitome of what a doctor should be.
–Susan Kreimer, New York
[You have] opened the door to parenthood when [I] thought it was forever closed.
–Lara Cook, Ashburn, VA
Fibroids
The first thing you have to know about fibroids is that they are always benign. Approximately 80% of all women have fibroids. They are the most common reason for hysterectomy in the United States. But most women with fibroids need no surgery at all, and those who do require surgery certainly do not need hysterectomies.
Benign But Baffling
Although fibroids are very common, no one knows what causes them. They are muscle tumors that originate in the wall of the uterus and grow under the influence of estrogen, the hormone all women produce everyday of their reproductive lives. We do know that a genetic error in the gene that controls the rate of replication for uterine muscle cells must be present for fibroids to develop.
In response to erroneous instructions from this gene, the uterine muscle cells begin to replicate at a tremendously accelerated pace, and before long, the cells begin to pile up on themselves as tiny seed-like growths. Eventually, the additional cells can no longer be incorporated into the body of the uterus. At some point in this process, the cells lose their identity as normal-looking muscle cells and become fibroids.
The genetic error responsible for fibroid development appears to be inherited, since fibroids usually run in families. For reasons no one understands, fibroids are most common among Afro-American and Jewish women.
The Estrogen Connection
When women are in their forties, their fibroids may undergo a growth spurt in response to a change in hormone balance. At this time in your menstrual life, you often produce more estrogen than normal, because progesterone, the ovarian hormone that inhibits the effects of estrogen, is diminished. Some doctors may see this common fibroid growth as an indication for surgery and will needlessly alarm patients with the news that "we have to do something, your fibroids are growing rapidly."
Once you understand that this hormonally stimulated growth can be considered normal at this stage of life, you will see that there is no cause for concern. At menopause, when the ovaries stop producing estrogen, fibroids will stop growing. In time, they may shrink and, sometimes, disappear.
Finding Fibroids
Usually fibroids cause no symptoms at all and most women have no idea they have fibroids until a doctor discovers the growths in the course of a pelvic examination. Because fibroids are so common, any physician who routinely performs pelvic exams should be able to diagnose them based on the position, size, and contour of the uterus.
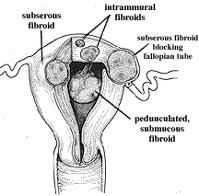
Although fibroids may cause no symptoms regardless of location, their placement often determines what kind of symptoms develop. Subserous fibroids (those on the outer surface of the uterus) typically are associated with the feeling of pressure. Intramural fibroids (those within the uterine wall) may cause pain, while submucous fibroids (those on the inner wall of the uterus) are associated with excessive menstrual bleeding.
A gynecologist usually can give you a pretty accurate approximation of the size of your fibroids. Because they are embedded in the wall of the uterus, as they grow, fibroids enlarge the entire uterus. Normally the uterus is the size of a pear. However, comparing fibroid size to the expansion of the uterus during pregnancy is much more precise. Thus you may have been told that your fibroids have enlarged your uterus to the size it would be if you were six to twelve weeks pregnant or more.
If a doctor isn't sure on the basis of a pelvic exam that what he or she is feeling is a fibroid, an ultrasound examination (sometimes called a sonogram) can provide more information. From the patient’s point of view, this is a simple, painless test during which a wand that emits sound waves is passed over the abdomen. The sound waves reflect back in the same way radar or sonar does. The pattern they make is analyzed by a computer, which projects a black-and-white television image of the area being examined. Ultrasound can confirm fibroids are present and can also provide information about size, location, and number.
A newer type of ultrasound exam involves beaming the sound waves through a wand inserted in the vagina. This test, trans vaginal ultrasound, may be performed in conjunction with traditional ultrasound to check behind the uterus for other fibroids or, sometimes, to examine the ovaries if they have been pushed out of place or hidden by large fibroids.
CA-125
A disturbing new trend has been creeping into the fibroid story. More and more women who have come to consult me for second opinions tell me that their doctors have ordered a blood test for a biochemical marker called CA-125 and suggested, based on the results, that there is the possibility of ovarian cancer. This is a reprehensible new tactic, which I believe is designed to scare women into surgery. CA-125 levels sometimes do rise among women with ovarian cancer, but they also can be elevated among women with fibroids and a number of other benign conditions, including normal menstruation. To confuse matters further, CA-125 levels may be normal among women who do have ovarian cancer. For this reason, the test is worthless as a diagnostic tool for ovarian cancer.
As matters now stand, CA-125 is useful only as a means of monitoring women who are being treated for ovarian cancer. Among these patients, normal CA-125 levels indicate that the cancer is under control, while elevated CA-125 tells doctors that the cancer has recurred. In any other circumstances, a test for CA-125 is meaningless.
Troublesome Fibroids
When fibroids cause heavy bleeding or pain, interfere with pregnancy, or are pressing on adjacent organs and interfering with their normal function, surgery may be the best treatment available.
Bleeding
 Fibroids can cause extremely heavy periods, which can continue for seven to fifteen days. As you know, every month the lining of the uterus thickens in preparation for pregnancy. When pregnancy does not occur, this tissue, the endometrium, is shed during menstruation. When the endometrium breaks away from the inner wall of the uterus, a network of corkscrew-shaped arteries called the spiral arteries open and begin to bleed. (The illustration shows a cross-section of uterus with the cavity filled with endometrium and the spiral arteries leading to the endometrium. The illustration shows some of the endometrium breaking away from the wall and the spiral arteries open and bleeding.)
Fibroids can cause extremely heavy periods, which can continue for seven to fifteen days. As you know, every month the lining of the uterus thickens in preparation for pregnancy. When pregnancy does not occur, this tissue, the endometrium, is shed during menstruation. When the endometrium breaks away from the inner wall of the uterus, a network of corkscrew-shaped arteries called the spiral arteries open and begin to bleed. (The illustration shows a cross-section of uterus with the cavity filled with endometrium and the spiral arteries leading to the endometrium. The illustration shows some of the endometrium breaking away from the wall and the spiral arteries open and bleeding.)
The bleeding is normal. It is designed to flush the tissue out of the uterus. The separation of the endometrium from the uterine wall releases a powerful hormone called prostaglandin, which causes the smooth muscle of the uterus to contract and squeeze the lining and blood out from the cavity and through the vagina. The contraction also squeezes shut the spiral arteries, stopping the bleeding. Under normal circumstances, women stop bleeding after a few days and do not hemorrhage or form clots.
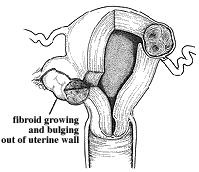
 If you look at the illustration to the right, which shows a submucous fibroid bulging into the cavity of the uterus, you can see that the uterine musculature cannot contract in the area surrounding the fibroid because the normal tissue has been pushed aside. As a result, the arteries in this area will remain open. When this occurs, a women will hemorrhage, pass large clots, and have a period that lasts up to fifteen days. She can become severely anemic and often will feel weak, faint, and unable to go about her usual activities. The longer this continues, the worse it becomes, because as the tumor grows, more spiral arteries become involved and the heavier she will bleed.
If you look at the illustration to the right, which shows a submucous fibroid bulging into the cavity of the uterus, you can see that the uterine musculature cannot contract in the area surrounding the fibroid because the normal tissue has been pushed aside. As a result, the arteries in this area will remain open. When this occurs, a women will hemorrhage, pass large clots, and have a period that lasts up to fifteen days. She can become severely anemic and often will feel weak, faint, and unable to go about her usual activities. The longer this continues, the worse it becomes, because as the tumor grows, more spiral arteries become involved and the heavier she will bleed.
Infertility
Every gynecologist knows of a woman with large fibroids who became pregnant and delivered a normal child. But those of us who specialize in infertility recognize that this depends upon the location and the size of the fibroids. Many patients with fibroids either cannot get pregnant or will not be able to sustain the pregnancy. To understand the obstacle fibroids present, you have to picture the scenario that sets the stage for a successful pregnancy.
A fertilized egg cannot implant in a section of the uterine wall occupied by a fibroid; if it tries to attach itself, it will be rejected immediately and flow out with the next period.
The fertilized egg may implant in the wall near a fibroid but far enough away so that it can connect with the mother's blood supply. Trouble begins when the nearby fibroid begins to grow in response to the tremendous amounts of estrogen women produce during pregnancy. At some point, the fibroid and the fetus will begin to compete for the available blood supply.
The fragile fetus, attached to the uterine wall only by a delicate thread, always loses this struggle to the tough fibroid rooted in the uterine wall. As a result, the pregnancy ends, usually within twelve weeks. If the fertilized egg implants farther away from the fibroid and establishes itself, it may have adequate blood supply but eventually it too will have to compete for space with the rapidly growing fibroids. As with the fetus located closer to the fibroid, the fetus will lose. Under these circumstances, a miscarriage usually occurs later in the pregnancy, between the fifteenth and eighteenth week.
Fibroids can interfere with pregnancy when they are located near the fallopian tubes and obstruct the tubes so that sperm cannot go up or the egg come down.
For many years gynecologists believed that only submucous fibroids interfered with pregnancy. However, a number of recent studies have demonstrated that women who were previously unable to conceive also became pregnant after intramural of subserous fibroids were removed.
Pain
Several types of pain associated with fibroids usually lead to surgery:
- Acute pain that occurs when a section of a fibroid undergoes degeneration (when a portion of the fibroid dies)
- Severe menstrual pain
- Pain from endometriosis, which is often associated with fibroids
- Severe pressure, tugging, and pulling sensation.
Surgery for Fibroids
When recommending hysterectomy, doctors sometimes use scare tactics – the suggestion that you may have cancer. A woman with fibroids is no more at risk for any kind of cancer than any other woman. Any time a doctor suggests the possibility of malignancy to justify hysterectomy, your best course of action is to find another doctor. Don’t let yourself be frightened into an unnecessary hysterectomy. If you have fibroids and need surgery, the appropriate operation is myomectomy, not hysterectomy.